
I find myself lost in numbers, my emotions dulled in order to absorb rising and falling fertility rates and changing percentages of unmet need for contraceptives. I’ve spent the last six months plowing through the public health literature on family planning, most of which seems to suggest that the greatest need for funding and support is in Sub-Saharan Africa. Other locations, including Latin America, “have it under control.” Have it under control? What does that mean? I was astonished to read this, because I have spent the past two decades working and studying in Latin America. I’ve sat and watched novelas alongside pregnant teenagers who dropped out of school, and I’ve taken cafecito with mothers in their homes while older children watched younger children running in and out and none of them wearing shoes. Still, numbers don’t lie. Fertility rates are dropping across Latin America and Asia. They remain high in Sub-Saharan Africa. If we strictly follow the numbers, we should focus our energies there.
Still, let me offer the story of one young couple to highlight my continued concern for Latin America. This is the story of Ishmael and Isabel. Ishmael lives in the burgeoning village of Santiago Atitlan, perched lakeside, surrounded by volcanos in the Guatemalan countryside. He comes from an indigenous Maya family; both of his parents speak only Tz'utujil, which suggests that they are illiterate. Nonetheless, Ishmael struggled to learn Spanish, and his parents supported him to stay in school (as well as his siblings). When he graduated high school, Ishmael gained entrance to university in Guatemala City, and he left to study mechanics to become an automotive engineer. At the time he had a girlfriend, whom he kept a secret, because his culture does not allow for dating. There is only marriage, or nothing. At the time, Ishmael swore that he did not need birth control because, well, he and his girlfriend weren’t doing anything like that.
Fast forward a year or two, and Ishmael confesses that he has gotten his girlfriend, Isabel, pregnant. Ishmael is terrified of what will happen next and what will happen to the future for which he has worked so hard. To his parents’ surprise, Isabel is a very modern young woman. She also is from Santiago, born to Maya parents, but she speaks near-perfect Spanish, dresses well, negotiates the city, deftly utilizes her cell phone, and is nearing the end of her training to be a primary grade teacher. Now her future is on the line too.
Maya custom prescribes that Isabel will move in with Ishmael’s parents, and this happens without question. Ending the pregnancy is not considered, nor is the couple’s union. A baby will fairly easily be absorbed into Ishmael’s family—the young mother will breastfeed, and then there need be only a few extra tortillas, some extra beans and vegetables, and some hand-me-down baby clothes. This is the way it goes.
It turns out that the most controversial question concerns where to wed. Ishmael is Catholic, and Isabel is Evangelical, and neither family will concede to a wedding in the other’s church. A wedding by law is considered utterly unimportant. And so the families argue and argue, until they agree to disagree and there will be no marriage, just a union.
The young couple worries about their studies, but their parents know the answer. Following Maya custom, Isabel’s parents have transferred the responsibility for her care to her husband’s family. She lives with them now, and her family will no longer pay for her school expenses. Ishmael knows that he will be a father and living in Guatemala City, and seven-to-eight hours away by bus is too difficult. Besides, his new wife has never been to Guatemala City and it is too foreign and ladino for her. He decides to transfer his studies to Xela, to the university branch there. Xela is only a few hours away by bus and far friendlier to indigenous ways. He can come home on the weekends when he has time.
In talking with Ishmael and Isabel, both were utterly surprised by the pregnancy. Isabel, in fact, did not realize she was pregnant until late, and she only told Ishmael at the fifth month. Both of them understood how sex could lead to pregnancy, but Isabel insisted that she had not known about birth control. Even if she had known, it’s unclear whether she would have felt comfortable discussing birth control with Ishmael or procuring it on her own. Ishmael had not suggested it, but his world now did not seem to be entirely changed by the union with Isabel or impending fatherhood. He would continue to live apart and study. When asked what they planned to do to prevent another baby, neither partner had an idea, although they didn’t seem too concerned either. Life had moved them forward, and they were taking what was presented to them.
This was a story told to me by a new gringo friend, who I met while visiting a clinic and midwifery group in Santiago recently. This friend had known Ishmael nearly his entire life, and he was frustrated by the turn that Ishmael’s life had taken and his own fatalistic response. I, too, am frustrated by the story of Ishmael and Isabel, because it is all too common around the world.
I struggle to know how to help. What would have motivated the young couple, and moreover, other couples, to use contraception?

During this trip to Guatemala, I conducted two focus groups with young women. I wanted to talk with them about family planning in their community. The answers I received, or, rather, didn’t receive, left me convinced that Latin America does not “have it under control.” Not by a long shot.
Admittedly, I went into the conversations with my expectations higher than I should have. The day prior, I had the good fortune to meet with more than a dozen women and girls involved in the Rxiin Tnamet, the local Tz'utujil-run village clinic attended by residents for health concerns that either are too serious to be treated by their curandero or not serious enough to need to visit the Hospitalito, the foreign-run hospital in town. Residents seem to like Rxiin Tnamet because it is staffed by locals who speak their language natively and understand their cultural practices and beliefs.

I was part of a group from the Global Fund for Women (GFW) visiting the clinic, which has received prior grants from GFW, and we had the chance to talk with (through an excellent interpreter) several of the female board members, midwives, adolescent village representatives, and girl counsel members. Rxiin Tnamet, led by Señora Leticia Toj (seen above) is steadfast in its commitment to the women’s movement, not only through the medical services it provides, but through its emphasis on community education and outreach and inclusion of all ages in its advisory boards and councils. Local communities even elect young girls, seen here wearing a crown, to represent their cohort at important council events.

While the girls on the village councils spoke confidently and intelligently about family planning, they were the exception, not the norm. As an anthropologist, I have conducted dozens of focus groups and semi-formal group interviews. I consider myself skilled at establishing rapport and getting even the most timid or dubious subject to crack a smile and offer over a morsel of information. These girls, however, were nearly impervious to my efforts. Group interviews should be spaces for gentle data gathering, a place to try out ideas and foster conversation. Rarely does the interviewer get to pick subjects in any scientific way. In my case, the demographics of subjects weren’t what I had asked for, so my line of questioning had to shift. I couldn’t tell any of my self-deprecating sex jokes to break the ice among a group that included seven-year-old girls.

Instead, with this group (ages 7-14), we talked mostly about menstruation, a topic hot on their young minds. We also discussed their ideas about ideal family size, and best ages for marriage and first pregnancy. These conversations led to some very interesting information, such as the girls’ belief that only two or three children are best (a decade ago that number would have been much higher), they wanted to be 18 before they married (no one said younger), and they thought 25 was a good age to have a first child (answers ranged between 19 and 30).

More in line with my interest in family planning was the discussion among pregnant adolescents (ages 16-26). The young women had just finished a class on fetal development at the Rxxin Tnamet clinic, and their instructor asked them to stay in order to participate in my interview. The half dozen adolescents obeyed, accompanied by two other women (already mothers) in their late forties. To begin, I encouraged them to form a cozy circle with their chairs. They did so silently, and continued to stare straight ahead. I got the sense that they were looking everywhere but at me, and thinking about everything except family planning.
Following introductions, I opened with a general question, did they know about birth control? “Sí, existen métodos,” one woman said. “Antes no habían de éstos.” (Yes, there are methods. Before there weren’t these kinds.) I could tell immediately that the coldness of this situation would require more specific questions. The young women felt no kinship with me. They were there out of good manners, nothing more.
“Have you thought about whether you will use birth control in the future, after your babies are born?” I asked.
Silence.
“How will you cuidarse (take care of yourselves)?” I asked, phrasing the sentence with softer words.
Silence, still, and eyes staring out the window.
If I wanted any kind of real data, I would have to give up hope of a chatty conversation. Instead, I asked the young women to list methods known to them. “Who here knows of a method that someone they know uses?” I asked. And so it went. Painstakingly, the women listed four methods: pills, injections, condoms, and the collar--a traditional rhythm method that looks a bit like a rosary. No one knew anyone who used the collar. Regarding condoms, “tal vez usan,” (maybe someone uses them), a woman suggested, but none of the women could tell me where to purchase condoms or whether they were expensive or cheap, suggesting a total lack of familiarity.
Pills and injections seemed less intimidating. One of the older women had used an injection years ago, and two of the young women knew friends who had used each method, although they had experienced side effects. Calores (hot flashes) or simply enfermedades (illness) were the side effects mentioned, and all of the women seemed satisfied with those responses.
I made the mistake of asking the adolescents if they lived at home, and if they spoke with their mothers about their pregnancies. “Sí, con mi mamá,” they all dutifully replied one right after the other. I hoped that it was true that they spoke with their moms. Changing my tactic, I asked who the first person was that they told about their pregnancies. For the briefest of moments, one woman smiled. She looked at me and said, “Con mi amiga,” (with my friend.) Of course! Suddenly the girls seemed to open up. Several explained that they told friends first of their pregnancies.
Feeling more positive, I returned to the topic of birth control. “Where did you all learn about birth control? Who taught you about sex and pregnancy?” I asked.
“From the radio,” one young woman replied. I was surprised. I hadn’t expected that answer.
“Really?” I asked.
“Sí,” another young woman confirmed. “From advertisements. And on TV,” she added.
“So, not in school?” I asked. I quickly added, “Wait, how long did each of you study?” The women had stayed in school between primary and middle school, and none had received any sexual education classes.
“We talk with friends about getting pregnant,” a young woman reiterated. “And en la calle (in the street).”
“So if you could have gone to a friend and gotten birth control, would you have used it?” I dared to suggest to the group. I looked at all of them, waiting for someone to answer. No one did. I tried again. “What if you could use your cell phone to text someone anonymously and ask them questions about birth control or pregnancy. Would you do that?” I had to clarify what I meant by anonymously, but, in the end, the young women seemed to like that idea very much. They hadn’t known it might be possible to get health information online, even though they all had smart phones.

In all, I was left with more questions generated by the interviews than I had answers. This community, if these girls and young women were at all an accurate representation, seemed to be in a state of transformation. They knew how they got pregnant. They knew modern contraceptive methods existed. They wanted small families and to marry later. But the women of reproductive age seemed utterly uninterested in family planning.
Literature that discusses poverty and development splits between 1) researchers who argue that people won’t change their lives if they don’t see a possibility for real change through concrete opportunities and 2) researchers who argue that people won’t be able to take advantage of opportunities until they have been able to take control of their lives in some small way, such as through the use of family planning. I swing back and forth in my stance. When a woman is surrounded by such tremendous fatalism, how can she decide to change her life? We can’t compel people to use family planning, so how will they ever take advantage if they see no real benefit? And, it seems, that even when they have something to lose, like Ishmael and Isabel, too often young people still make poor decisions for themselves.
This most recent trip to Guatemala reminded me that family planning investment is needed worldwide, not just where the numbers point. We need to seek creative solutions, that derive from conversations with local people facing these problems on the ground. Only solutions that derive from their lived experiences will be attractive and sustainable long-term.

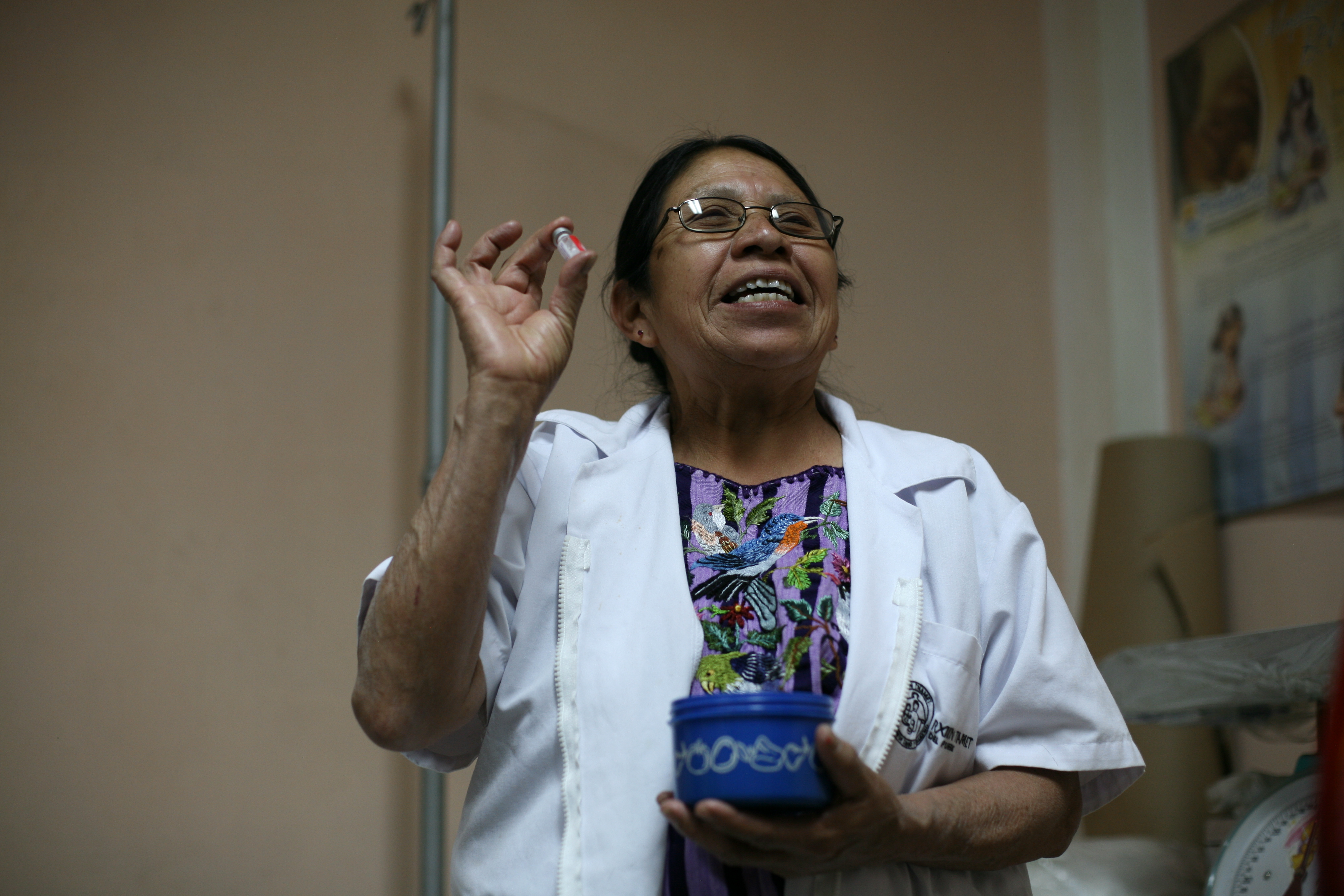
During this field trip to Santiago Atitlán, I was struck most by the nurse at Rxxin Tnamet. I didn't catch her name, but she has been working at the clinic since its founding, decades ago. Her enthusiasm for birth control was catching as she showed us the nondescript tupperware container where she stores and encourages other women to store their contraceptives of choice.
If only we could figure out how to connect her enthusiasm with young women's insecurity and fatalism in order to break down the barrier of unmet need. I know that the women who staff this clinic are trying every day to make this happen. It's certainly top of my mind these days.